What Diagnostic Laboratories Must Demand From a Clinical LIMS: A Practical Guide to Sample Integrity, Compliance and Turnaround Time
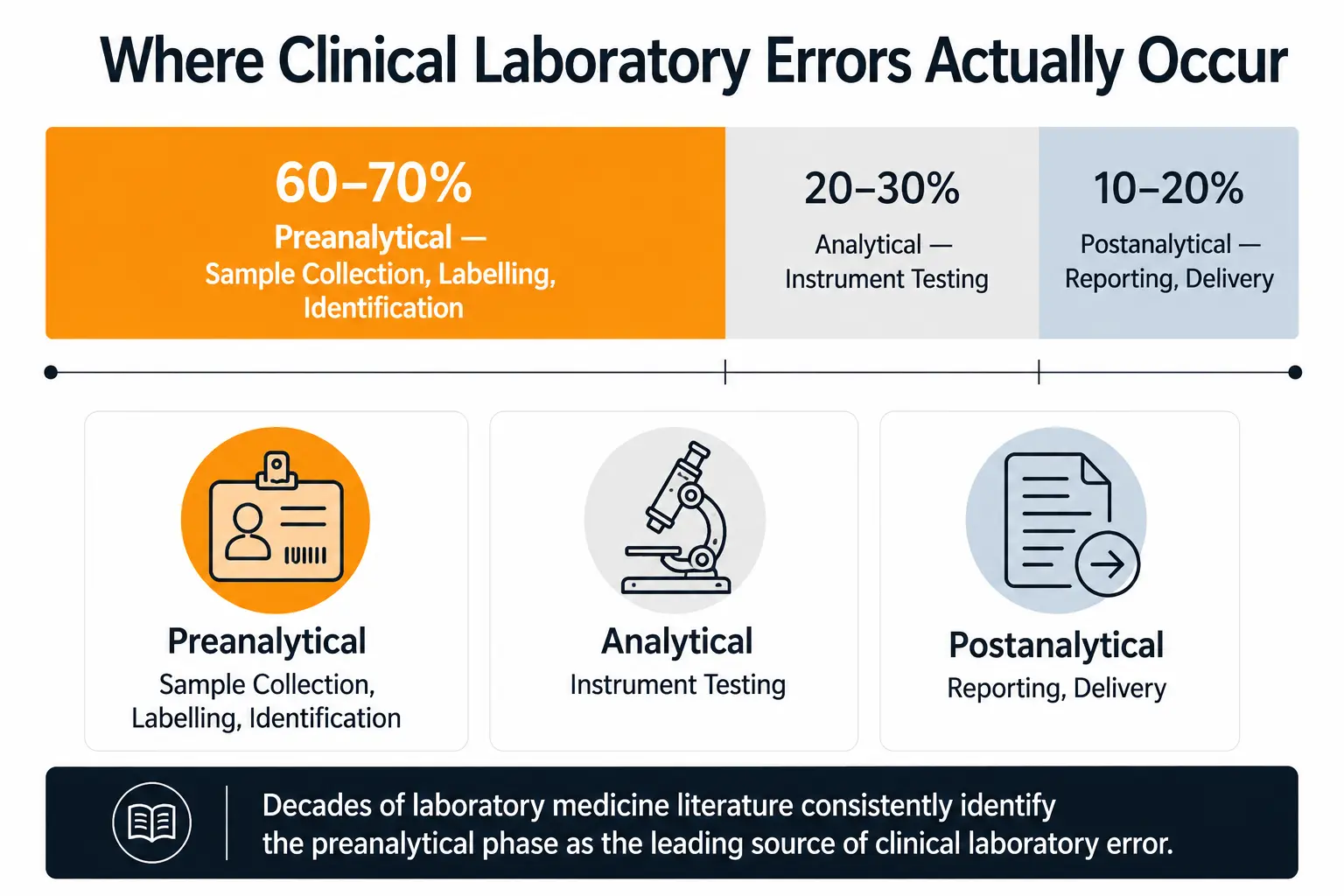
A review of decades of established clinical laboratory quality literature reveals a consistent, heavily documented finding: the vast majority of clinical laboratory errors do not occur during the analytical testing phase. Extensive research, including repeated College of American Pathologists (CAP) Q-Probes studies and foundational peer-reviewed laboratory medicine research, has demonstrated that up to 70% of all clinical laboratory errors occur in the preanalytical phase. Specifically, these errors are concentrated in specimen collection, labelling, and identification.
In the United States, all clinical laboratory testing performed on human specimens for health assessment or the diagnosis, prevention, or treatment of disease is governed by the Clinical Laboratory Improvement Amendments (CLIA). Globally, ISO 15189 serves as the internationally recognized standard for medical laboratory quality and competence. Furthermore, CAP accreditation layers highly stringent, discipline-specific proficiency testing and quality management requirements on top of these baseline regulatory frameworks.
Despite these rigorous frameworks and the introduction of highly advanced analytical instrumentation, the data remains uncompromising: the majority of documented laboratory errors are not analytical failures. They are identification and data management failures. When an incorrect diagnosis is issued based on a perfectly executed diagnostic test performed on a mislabeled sample, the analytical precision of the instrument is rendered entirely irrelevant.
A clinical diagnostics LIMS exists specifically to close this gap — to make sample identification, instrument data capture and reporting a function of system architecture rather than manual vigilance.
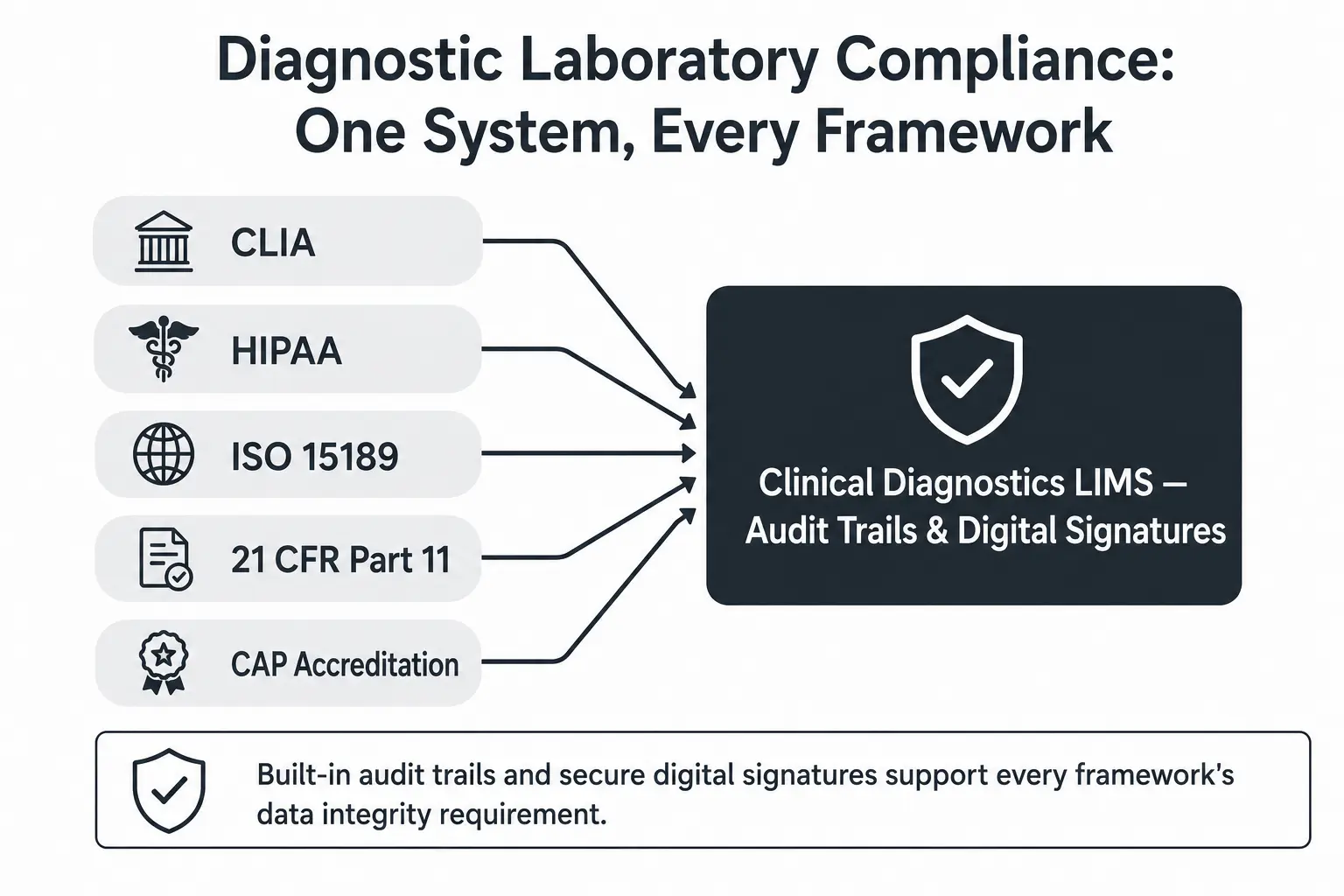
The exact category of failure that leads to patient safety events is the category that a laboratory's data management infrastructure is primarily responsible for preventing. This practical, factual guide breaks down exactly what a diagnostic laboratory's data management system must provide to mitigate these risks. It details how specific, verifiable software capabilities directly map to the regulatory frameworks — CLIA, HIPAA, ISO 15189, 21 CFR Part 11, and CAP — that diagnostic laboratories must satisfy to maintain their accreditation and protect patient safety.
TL;DR: Quick Summary
- Capability Domains Covered: Barcode-based sample tracking, instrument integration, workflow automation, real-time reporting, detailed turnaround time analytics, and secure remote multi-site access.
- Compliance Coverage: Detailed mapping of system capabilities to CLIA operational requirements, HIPAA data privacy, ISO 15189 quality standards, 21 CFR Part 11 electronic records, and CAP accreditation checklists.
- Central Factual Claim: Clinical laboratory quality literature explicitly documents that sample identification integrity and preanalytical data management, not analytical instrument precision, represent the leading categories of clinical laboratory error.
What Is a Clinical Diagnostics LIMS?
A clinical diagnostics LIMS is a specialized laboratory information management platform designed for diagnostic facilities that manages the complete patient sample lifecycle from barcode-based collection through instrument-integrated testing to physician and patient reporting. It is fundamentally differentiated from generic laboratory software by its rigid compliance architecture, which is specifically engineered to satisfy CLIA, HIPAA, ISO 15189, 21 CFR Part 11, and CAP accreditation requirements through built-in audit trails, secure digital signatures, and strict role-based access controls.
What This Article Covers
- The Preanalytical Error Challenge: Why sample identification is the most documented vulnerability in clinical diagnostics.
- Barcode-Based Sample Tracking: How automated logging secures the chain of custody from accessioning to archiving.
- Instrument Integration: Eliminating transcription risk across testing disciplines from molecular diagnostics to microbiology.
- Regulatory Compliance Architecture: Mapping software capabilities directly to CLIA, HIPAA, ISO 15189, and CAP requirements.
- Turnaround Time (TAT) Analytics: How real-time reporting and detailed monitoring accelerate clinical decision-making.
- Secure Remote Collaboration: Leveraging cloud architecture, SOC 2, and ISO 27001 standards for multi-site laboratory networks.
- FAQs
1. Why Is Sample Identification the Central Challenge in Diagnostic Laboratories?
To understand the architecture of a modern clinical diagnostics LIMS, one must first understand the specific operational vulnerabilities it is designed to mitigate. The challenge of sample identification is heavily documented across clinical laboratory literature.
The Dominance of Preanalytical Errors
Peer-reviewed studies and continuous quality improvement data indicate that specimen mislabeling, patient misidentification, and manual transcription errors represent the dominant category of clinical laboratory error. These events occur primarily before the sample ever reaches the analytical instrument.
"In a diagnostic laboratory setting, a mislabeled sample does not simply produce an inaccurate report; it produces an accurate result attributed to the wrong patient, directly resulting in erroneous diagnoses and inappropriate clinical interventions."
This distinction matters more in clinical diagnostics than in almost any other laboratory sector. If an environmental water sample is mislabeled, a facility might fail a municipal compliance check. If a surgical pathology biopsy or a critical molecular diagnostic blood draw is mislabeled, a patient may receive a catastrophic false-positive diagnosis or be denied life-saving treatment due to a false-negative result attached to their medical record.
Removing the Manual Transcription Step
Barcode-based, automated sample logging directly addresses this specific, documented failure mode. By integrating barcode technology, the laboratory removes the manual transcription steps where preanalytical errors are mathematically shown to concentrate. Instead of a technician reading a handwritten label and typing a patient identifier into a testing queue, a scanner electronically captures the data, ensuring absolute fidelity between the physical specimen and the digital patient record.
2. What Does Barcode-Based Sample Tracking Actually Provide?
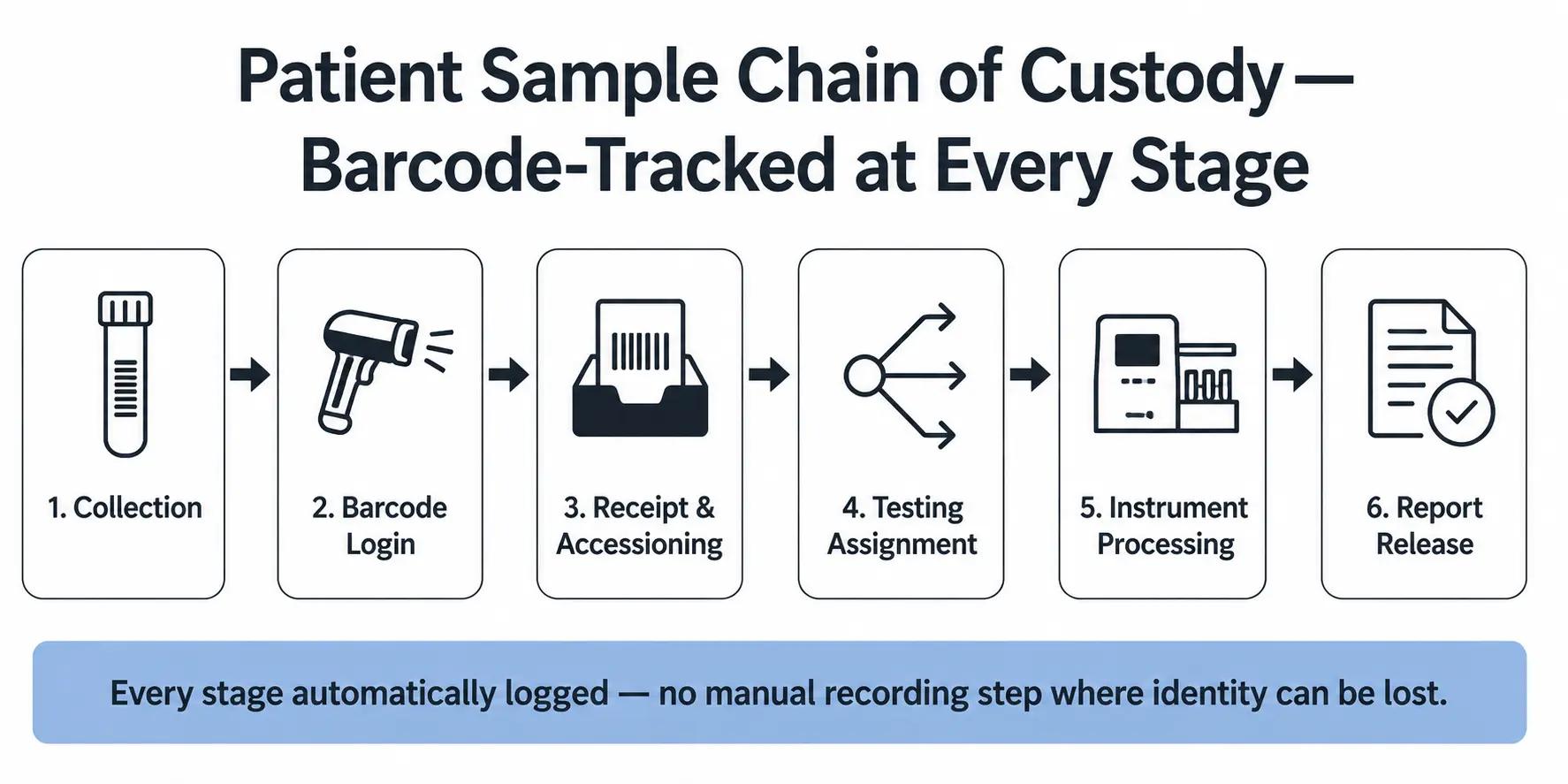
Implementing barcode integration in a diagnostic laboratory is not merely about printing labels; it is about establishing an unbroken, auditable chain of custody that spans the entire facility.
The Operational Reality of Automated Sample Logging
Genuine barcode integration means tracking a patient sample through every single step of the diagnostic process. When a sample arrives at the laboratory, scanning the barcode instantly logs the sample receipt, time-stamping the exact moment it enters the facility's custody.
As the sample moves from receipt to accessioning, through various processing benches, into testing, and finally to storage or disposal, every movement is automatically logged rather than manually recorded on paper tracking sheets.
Traceability for CLIA and ISO 15189
This level of automated sample logging provides immense, measurable value for regulatory compliance. Both CLIA and ISO 15189 stipulate rigorous requirements around sample chain of custody and traceability. Assessors require laboratories to demonstrate exactly who handled a sample, what was done to it, and when that action occurred.
When barcode scanning governs sample movement, this traceability is generated automatically in the background. If a CAP inspector requests the complete history of a specific patient specimen from three months prior, the laboratory manager can retrieve a comprehensive, timestamped digital ledger in seconds, definitively proving the integrity of the sample's handling.
3. How Does Instrument Integration Support Diagnostic Testing Across Disciplines?
The analytical phase of diagnostic testing relies on a diverse, highly sophisticated fleet of laboratory equipment. However, if the data generated by these instruments must be manually typed into a reporting system, the laboratory is actively re-introducing the very preanalytical-adjacent risks it sought to eliminate.
Spanning Diagnostic Disciplines
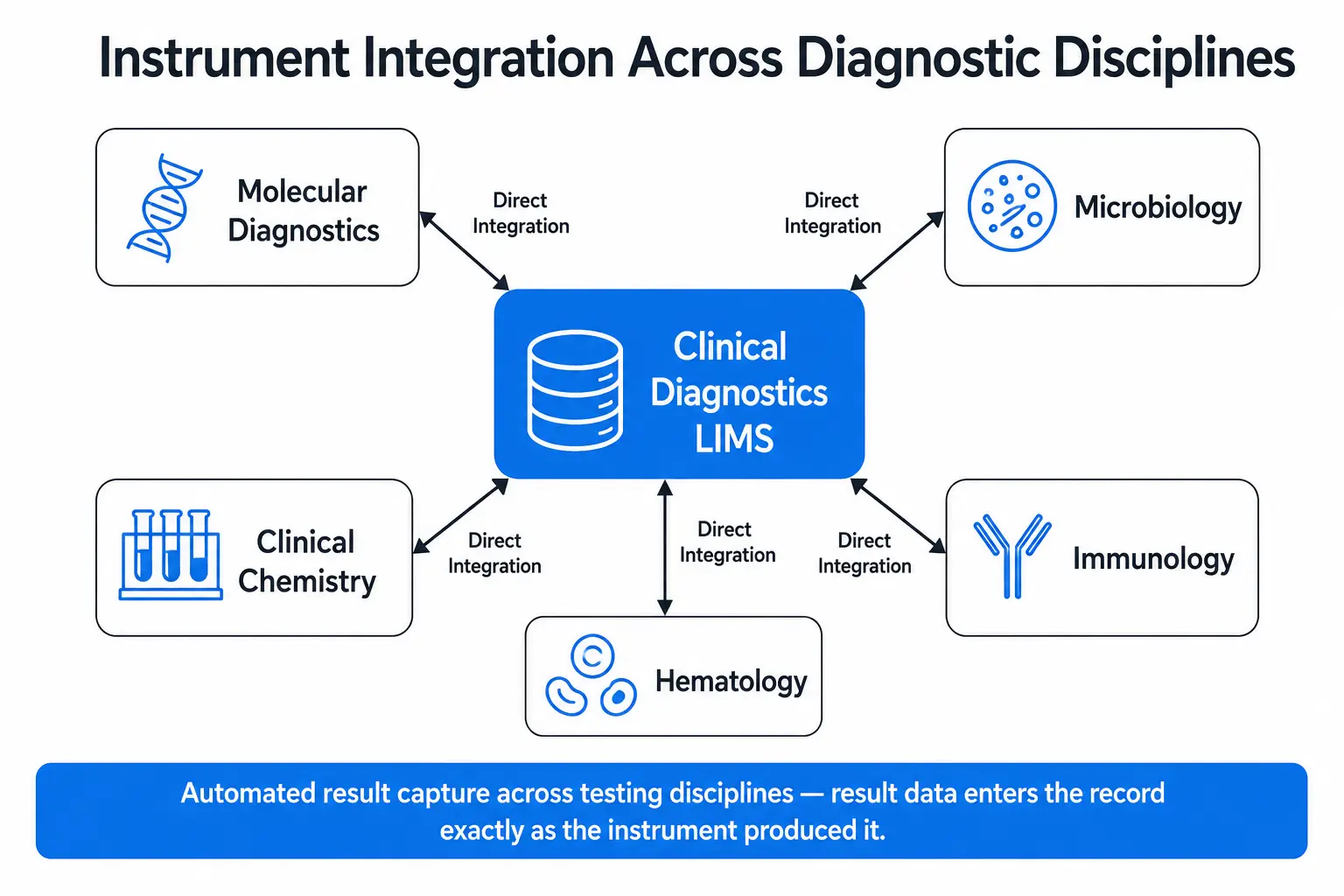
A robust diagnostic laboratory software platform must provide seamless integration with laboratory instruments and diagnostic equipment across a wide range of diagnostic testing disciplines.
This includes everything from high-throughput molecular diagnostics platforms executing complex PCR assays, to automated microbiology systems tracking culture growth, to standard clinical chemistry and hematology analyzers. The goal is complete, automated data entry. When an instrument completes its analysis, the result is pushed directly and instantaneously into the LIMS database, paired flawlessly with the barcode-scanned sample ID.
"Manual transcription of instrument results in a diagnostic context carries the exact same risk profile as sample misidentification. Direct instrument integration removes this critical risk at the point of data capture."
Eliminating Downstream Verification Risk
Relying on downstream human verification to catch manual transcription errors is a statistically flawed quality control strategy. Humans suffer from fatigue and expectation bias. Direct instrument integration eliminates this risk entirely. It ensures that the exact numerical value, qualitative finding, or graphical output generated by the diagnostic equipment is exactly what populates the patient's record, safeguarding diagnostic integrity across every testing discipline.
4. What Regulatory Compliance Must a Diagnostic LIMS Satisfy?
Diagnostic laboratories operate in one of the most heavily regulated environments in the healthcare sector. A clinical LIMS cannot treat compliance as an optional add-on; compliance must be the foundational architecture of the software.
CLIA (Clinical Laboratory Improvement Amendments)
CLIA governs all facilities in the U.S. that perform laboratory testing on human specimens for health assessment. CLIA inspections focus heavily on personnel competency, test method validation, and quality control records. A CLIA compliant LIMS automatically logs which technician performed which test, utilizing built-in audit trails to prove to inspectors that only personnel with documented, current competency were allowed to release patient results.
HIPAA (Health Insurance Portability and Accountability Act)
As laboratories handle vast amounts of Protected Health Information (PHI), a HIPAA compliant laboratory system is a strict legal requirement. The LIMS must protect patient data privacy and security through rigid role-based access controls, ensuring that users can only access the minimum necessary PHI required to perform their specific job functions.
ISO 15189
ISO 15189 is the gold standard for medical laboratory quality and competence globally. It demands exhaustive documentation of the laboratory's quality management system, continuous improvement metrics, and absolute data integrity. The LIMS supports this through its automated sample tracking and detailed analytics, providing the objective evidence of traceability and operational control that ISO 15189 assessors demand.
21 CFR Part 11
For diagnostic laboratories operating under FDA-regulated frameworks, compliance with 21 CFR Part 11 is mandatory. This regulation dictates the criteria under which electronic records and electronic signatures are considered trustworthy, reliable, and equivalent to paper records. The LIMS satisfies this through secure digital signatures and unalterable audit trails, ensuring that every result approval is irrefutably tied to an authenticated medical professional.
CAP Accreditation Requirements
CAP accreditation layers additional, highly specific proficiency testing and quality system requirements onto the laboratory. A CAP accreditation software platform aids compliance by enforcing configurable custom workflows. It ensures that the specific, CAP-mandated procedural steps for diverse disciplines — from molecular diagnostics to microbiology — are followed consistently for every single sample, with every step permanently recorded in the audit trail.
5. How Do Configurable Workflows and Automation Reduce Manual Laboratory Work?
The operational efficiency of a diagnostic laboratory is directly proportional to its ability to automate non-value-added administrative tasks. Highly trained clinical laboratory scientists should be evaluating complex diagnostic data, not performing repetitive clerical work.
Automating Repetitive Tasks
A world-class clinical LIMS delivers extensive automation of repetitive tasks. This includes the automated logging of sample receipt upon barcode scan, the automated routing of test processing instructions to the correct laboratory bench, the automated entry of results via instrument integration, and the automated generation of the final diagnostic report once all parameters are met and verified.
Configurable Custom Workflows
Because diagnostic laboratories encompass multiple distinct disciplines, a rigid, one-size-fits-all software workflow will inevitably fail. Molecular diagnostics workflows look nothing like microbiology workflows.
The LIMS must feature configurable custom workflows that allow the laboratory to design specific procedural paths for different test types. This capability ensures absolute consistency across diverse diagnostic processes — mandating specific quality control checks or review steps based on the test type — without requiring the laboratory to pay for custom software development for every new assay they introduce.
6. How Does Real-Time Reporting Improve Diagnostic Decision-Making?
In clinical diagnostics, the value of a perfectly accurate test result decays rapidly over time. The speed at which data is transformed into an actionable report directly impacts patient care.
Real-Time, Customizable Reporting
A primary function of a clinical LIMS is the generation of real-time customizable reporting that is easily shareable with healthcare providers and patients. Physicians require reports that highlight abnormal results clearly, present historical patient trending data, and provide clear reference ranges. The LIMS automates the assembly of these complex reports, formatting the integrated instrument data instantaneously upon final approval by the pathologist or laboratory director.
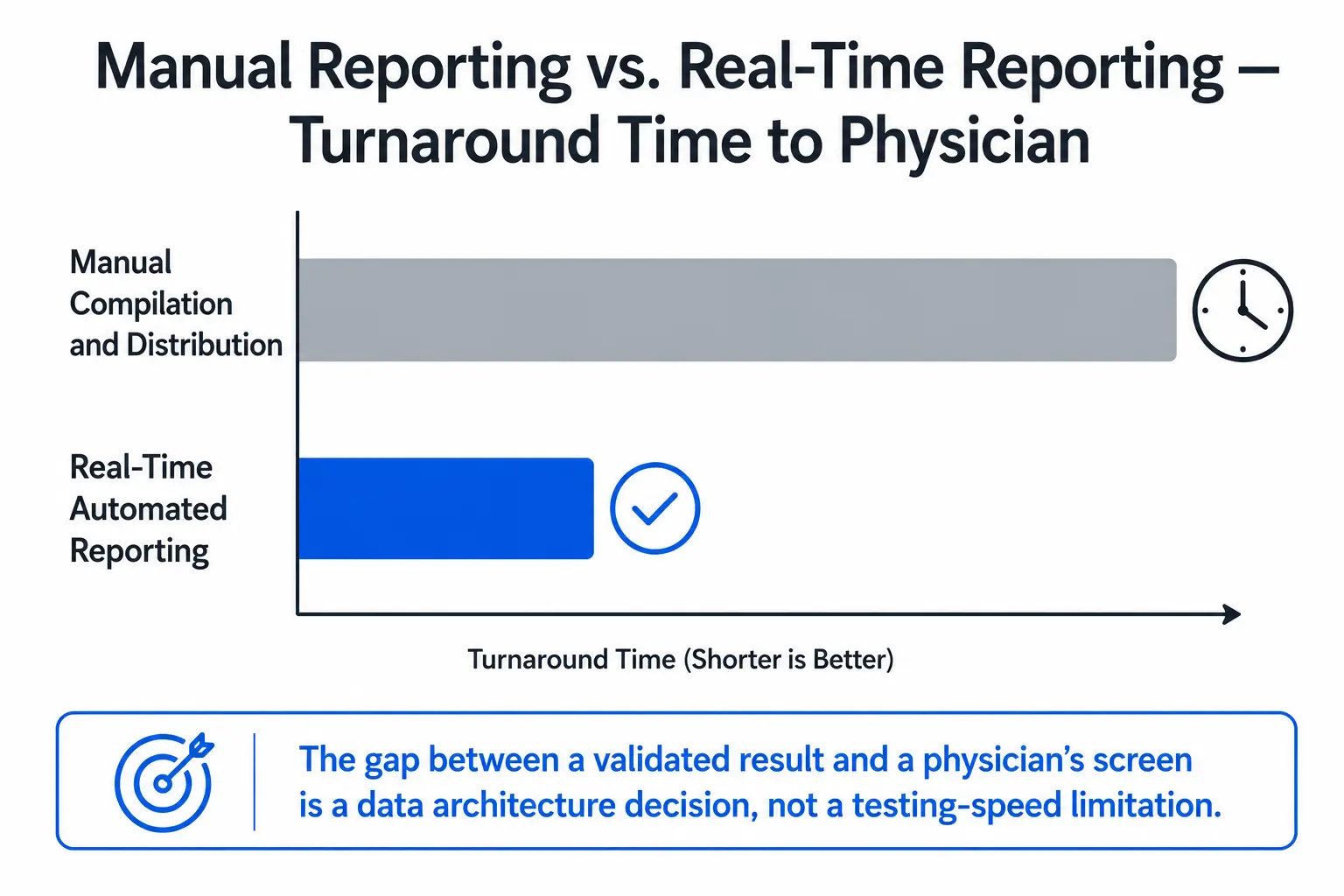
"In diagnostic medicine, turnaround time is a critical clinical metric. There is a direct, undeniable relationship between how quickly a validated result reaches a treating physician and the speed of clinical decision-making."
Detailed Analytics and Turnaround Time Monitoring
Beyond individual patient reports, the LIMS must provide detailed analytics and monitoring of the laboratory's operational performance. Turnaround Time (TAT) is one of the most closely monitored metrics in any diagnostic facility.
By functioning as laboratory turnaround time software, the LIMS tracks the exact duration between sample receipt and result reporting for every single test. This allows laboratory managers to identify bottlenecks, optimize staffing, and ultimately accelerate turnaround times, ensuring that critical diagnostic intelligence reaches healthcare providers faster.
7. What Does Secure Remote Access Mean for Multi-Site Diagnostic Operations?
Modern diagnostic laboratory networks frequently span multiple hospital campuses, reference facilities, and outpatient collection centers. Confining laboratory data to a local server is no longer a viable operational strategy.
Cloud-Based Collaboration
A modern clinical diagnostics LIMS provides secure cloud-based access from any location. This enables real-time remote monitoring of laboratory operations by off-site administrators and facilitates real-time collaboration between medical professionals and laboratories. A pathologist at a central reference facility can securely review and digitally sign off on test results generated by instruments at a remote satellite laboratory, drastically reducing geographical delays in patient care.
The Security Architecture Foundation
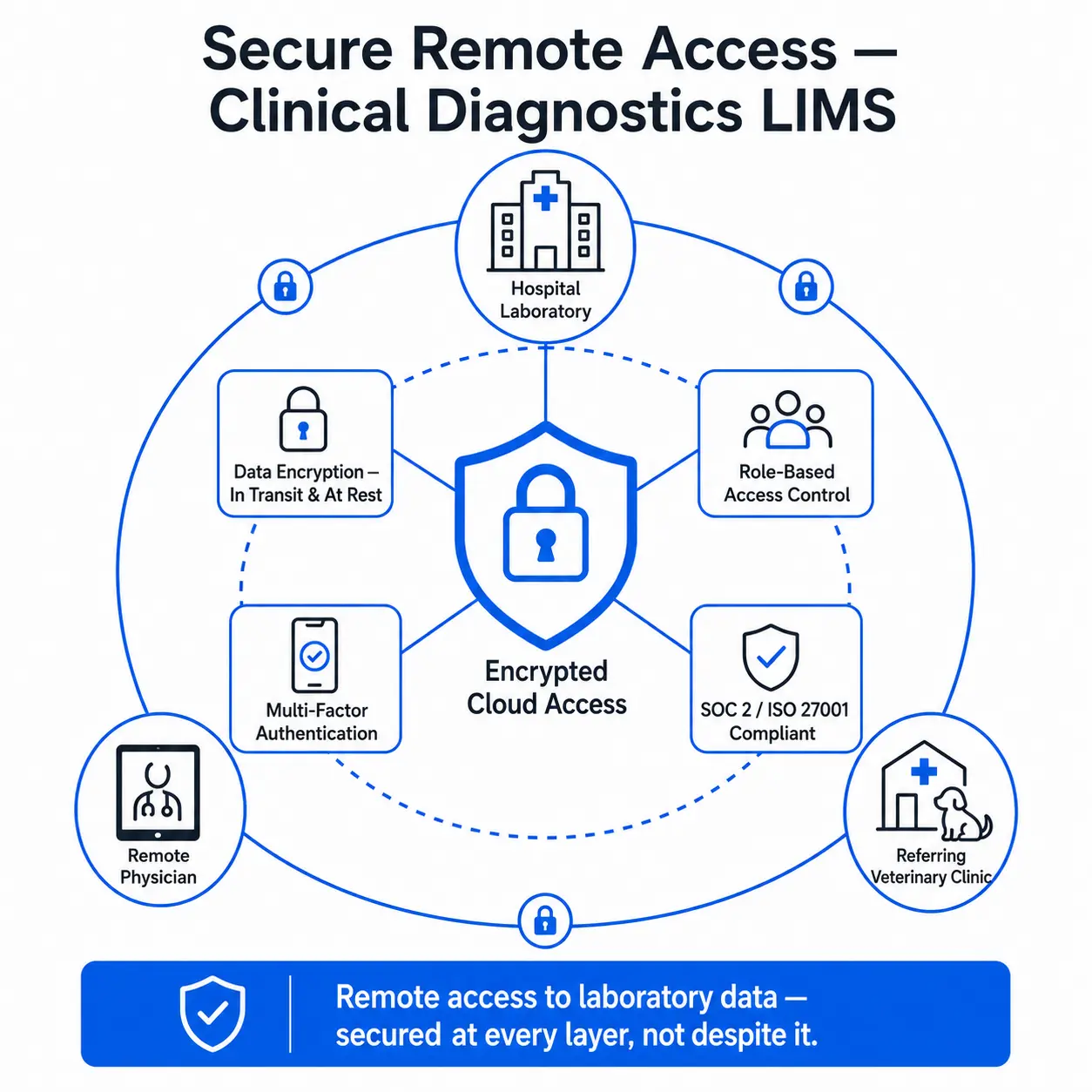
Remote access is only viable if it is fundamentally secure. The LIMS must be built on a rigorous platform security architecture. This includes:
- Data Encryption: All PHI and laboratory data must be encrypted both in transit and at rest.
- Role-Based Access Control (RBAC): Restricting data access strictly based on the user's verified job role.
- Multi-Factor Authentication (MFA): Ensuring that compromised passwords cannot lead to unauthorized system access.
- Automated Backups: Guaranteeing data preservation and disaster recovery capabilities.
- SOC 2 and ISO 27001 Compliance: Providing independent, third-party validation that the software vendor's security protocols meet the highest international standards for information security management.
Security Question for IT Teams: When evaluating cloud deployment, ask your vendor: "Can you provide a current SOC 2 Type II report and proof of ISO 27001 certification to validate your data encryption and backup protocols?"
8. Does the Same Framework Apply to Veterinary Diagnostic Laboratories?
When evaluating a veterinary diagnostic LIMS, laboratory directors often assume they require an entirely different category of software. Operationally, this is a misconception.
Veterinary diagnostic testing shares the identical underlying laboratory workflow challenges as human clinical diagnostics. A veterinary diagnostic facility processes blood, tissue, and fluid samples. They run clinical chemistry, hematology, microbiology, and molecular diagnostic panels. They rely on complex analytical instrumentation, and they must deliver accurate reports to referring veterinarians and animal owners quickly.
Therefore, the operational framework detailed in this guide applies directly to veterinary diagnostic laboratories. They require the exact same barcode-based sample tracking to prevent misidentification. They require the exact same instrument-integrated result capture across disciplines to eliminate manual transcription errors. They require the same configurable workflows to manage diverse testing panels, and they demand the same real-time reporting capabilities.
A high-quality clinical diagnostics LIMS handles veterinary workflows seamlessly, applying the same rigorous audit trails and data integrity standards to animal health testing. It is important to note, however, that while the software workflow is identical, species-specific reference ranges and regional veterinary regulatory requirements should always be evaluated and configured independently by the laboratory management team.
9. The Documented Cost of Manual Sample and Data Management in Diagnostics
The decision to implement or upgrade a clinical LIMS is frequently viewed through the lens of software procurement cost. However, maintaining a manual, fragmented, or legacy data management system carries severe, documented costs that directly impact laboratory viability.
The Clinical Risk Cost
As established in clinical laboratory medicine literature, preanalytical identification errors are the most frequent source of laboratory failure. The clinical risk cost of these errors is immense. Misidentified samples lead to misdiagnoses, unnecessary medical procedures, or delayed critical treatments. The liability and reputational damage associated with a single patient safety event caused by a transcription or labeling error vastly exceeds the cost of secure software infrastructure.
The Inspection Finding Risk
Laboratories operating under CLIA and CAP face rigorous, unannounced inspections. A primary focus of these inspections is the traceability of the sample and the competency of the personnel performing the test. In a manual system, producing complete, consistent chain-of-custody documentation across thousands of historical samples is nearly impossible. The cost of an incomplete audit trail is severe: inspection deficiencies, mandatory corrective action plans, or in extreme cases, the suspension of the laboratory's CLIA certificate.
"A laboratory's data management infrastructure is the primary control point for the exact category of error that clinical laboratory quality literature has identified as most significant."
The Operational Cost of Manual Transcription
When laboratory technologists are required to manually transcribe data from instrument printouts into a reporting system, the laboratory incurs a massive operational cost. Highly compensated clinical staff spend hours per shift performing data entry instead of analyzing complex diagnostic data. This manual transcription directly limits the total testing volume the laboratory can safely process per shift.
The Turnaround Time Cost
In diagnostics, time is a clinical asset. Manual report compilation and the physical or manual electronic distribution of results to referring physicians inherently delays patient care. When turnaround times lag behind industry benchmarks, healthcare providers will invariably route their diagnostic testing to competing reference laboratories that can provide real-time, automated reporting.
The Multi-Site Coordination Cost
For healthcare networks operating multiple laboratory sites, managing operations without a unified, securely accessible system of record creates extreme inefficiency. Standardizing testing protocols, sharing pathologist expertise across locations, and aggregating quality metrics becomes a labor-intensive, error-prone exercise rather than an automated, real-time management capability.
10. Generic LIMS vs. Clinical Diagnostics-Specific LIMS
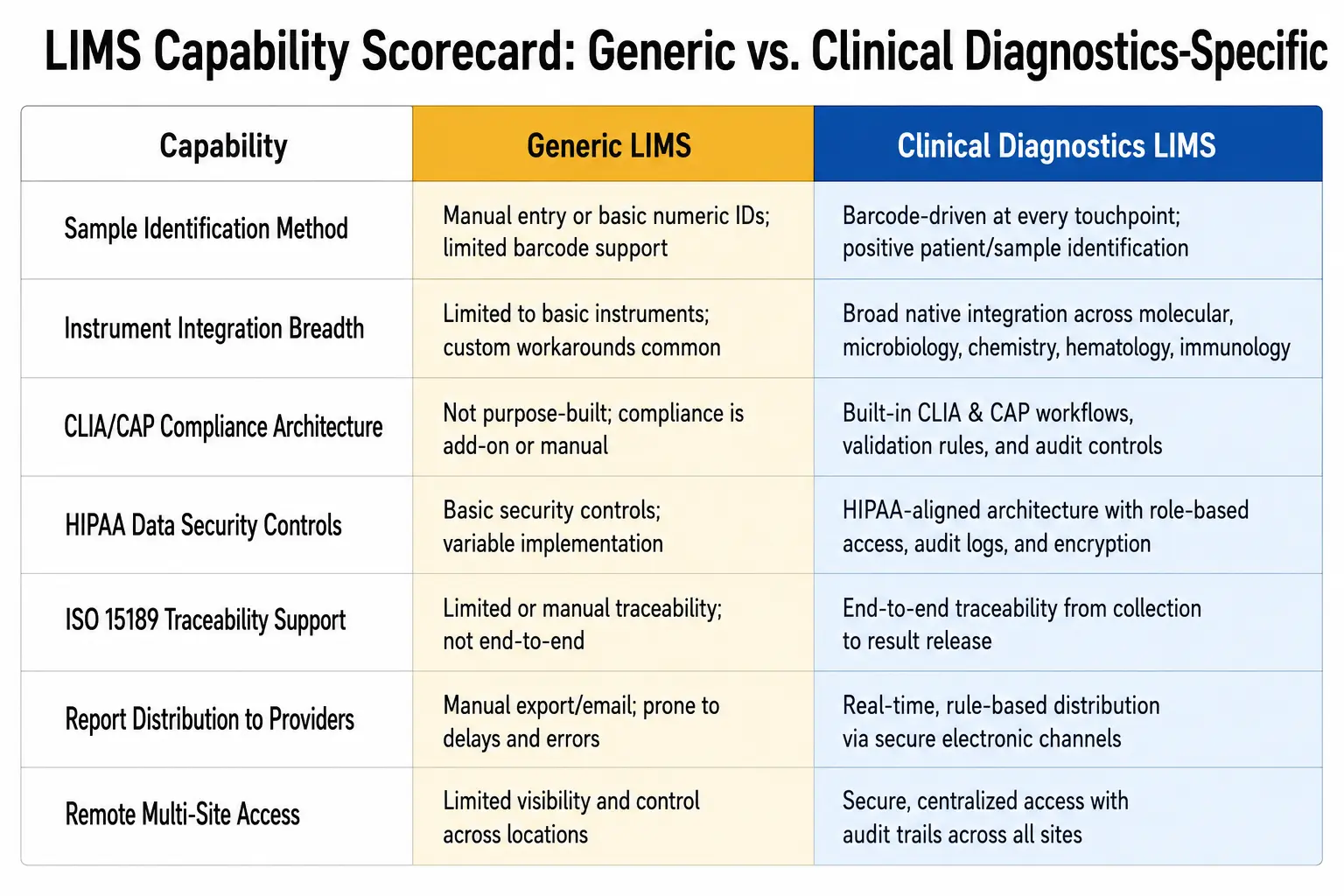
A generic laboratory system designed for manufacturing or environmental testing is fundamentally unsuited for the stringent demands of human health diagnostics.
| Capability Requirement | Generic Laboratory Software | Clinical Diagnostics LIMS |
|---|---|---|
| Sample Identification Method | Manual text entry or basic printed batch labels. | Integrated barcode scanning tracking the patient sample through every discrete diagnostic step. |
| Instrument Integration Breadth | Limited to basic CSV uploads or generic interfaces. | Seamless integration across diagnostic disciplines from molecular PCR platforms to microbiology systems. |
| CLIA/CAP Compliance Architecture | Basic user logins; compliance requires manual workarounds. | Built-in audit trails, secure digital signatures, and automated personnel tracking designed for clinical audits. |
| HIPAA Data Security Controls | Standard password protection; no PHI segregation. | Strict role-based access control, MFA, encryption, and SOC 2/ISO 27001 compliant architecture protecting PHI. |
| ISO 15189 Traceability Support | Static records lacking granular movement history. | Automated, timestamped chain-of-custody logging from sample receipt to final reporting. |
| Report Distribution | Static internal PDFs requiring manual emailing. | Real-time, customizable reporting shareable securely with healthcare providers and patients. |
| Remote Multi-Site Access | Often restricted to local on-premise networks. | Secure cloud-based access allowing real-time remote monitoring and multi-site professional collaboration. |
11. How Do You Evaluate a Clinical Diagnostics LIMS?
When selecting an ISO 15189 LIMS or evaluating your current diagnostic infrastructure, laboratory directors must move past general software demonstrations and interrogate the specific capabilities required for clinical compliance. You can also request a demonstration to validate these capabilities in a live environment.
- How deep is the barcode and sample identification workflow? Does the system merely print a label upon accessioning, or does it require a barcode scan to authorize sample processing at each specific laboratory bench, thereby ensuring absolute traceability?
- What is the true breadth of instrument integration? Can the vendor demonstrate seamless integration with the specific diagnostic equipment utilized in your facility? Does this integration span your diverse disciplines, effectively eliminating manual data entry for both molecular diagnostics and automated microbiology?
- Does the system natively support CLIA, HIPAA, ISO 15189, and CAP compliance? Are these compliance frameworks supported by the core architecture of the software, or does the vendor expect your laboratory to build custom workflows to satisfy inspection requirements?
- How are audit trails and digital signatures implemented? Are the audit trails immutable? Does the system utilize secure digital signatures for result verification that comply fully with 21 CFR Part 11 requirements for electronic records?
- What is the foundation of the remote access security architecture? If the system offers cloud-based remote access, is that access secured by role-based access controls, multi-factor authentication, and data encryption? Can the vendor provide SOC 2 and ISO 27001 certifications to prove it?
- Does the system provide visibility into report distribution and turnaround time? Can the system automate the generation of customizable reports, and does it feature detailed analytics dashboards that allow you to monitor and improve laboratory turnaround times in real-time?
FAQ: Frequently Asked Questions
How does barcode-based sample tracking specifically reduce CLIA inspection risk?
CLIA requires laboratories to maintain a positive identification of the specimen from collection through reporting, and to retain records of all processing steps. Barcode-based tracking automates this documentation. Every time a sample is scanned at a workstation, the LIMS generates a timestamped, immutable audit log detailing exactly who handled the specimen and when. This eliminates the risk of missing or illegible manual tracking logs during a CLIA inspection.
What diagnostic testing disciplines can instrument integration support?
A purpose-built clinical diagnostics LIMS is designed to interface with a vast array of analytical equipment. This includes high-throughput clinical chemistry analyzers, hematology platforms, complex molecular diagnostics equipment (such as PCR cyclers), and automated microbiology systems. By facilitating automated data entry across these disciplines, the LIMS ensures that transcription errors are eliminated regardless of the specific diagnostic test being performed.
How does a clinical diagnostics LIMS support HIPAA compliance specifically?
HIPAA mandates the strict protection of Protected Health Information (PHI). The LIMS supports this through a combination of data encryption (protecting data both in transit over networks and at rest on servers) and stringent Role-Based Access Control (RBAC). RBAC ensures that a laboratory technician only sees the specific patient data required to run their assigned test, while restricting broader medical record access exclusively to authorized pathologists and laboratory directors.
Can the same system serve both a hospital laboratory and a veterinary diagnostic laboratory?
Yes. The underlying laboratory workflows — sample accessioning, barcode tracking, instrument integration, and reporting — are identical. A robust clinical LIMS applies the same rigorous automation, audit trails, and quality control architectures to animal health testing as it does to human diagnostics. While the software platform is the same, the veterinary laboratory will simply utilize the system's configurable workflows to apply species-specific reference ranges and regional veterinary reporting requirements.
What does real-time reporting to referring physicians actually involve?
Rather than batch-printing physical reports or manually compiling PDFs to send at the end of a shift, real-time reporting leverages the LIMS automation. The moment a pathologist or laboratory director applies a secure digital signature to verify a test result, the LIMS automatically generates a customized report and makes it instantaneously available to the referring healthcare provider through secure, compliant sharing protocols, drastically reducing the time to clinical intervention.
How does remote access work without compromising CLIA or HIPAA data security requirements?
Secure remote access is achieved through strict adherence to enterprise security standards. The LIMS utilizes cloud-based architecture fortified by Multi-Factor Authentication (MFA), ensuring only verified users can log in. Data is encrypted end-to-end. Furthermore, compliance with comprehensive security frameworks like SOC 2 and ISO 27001 ensures that the cloud infrastructure undergoes rigorous, independent audits to verify that all PHI remains protected from unauthorized access, even during remote collaboration.
Key Takeaways
- Preanalytical Vulnerability: Up to 70% of clinical laboratory errors occur in the preanalytical phase; a LIMS specifically targets this vulnerability by eliminating manual identification and transcription.
- Traceability is Automated: Barcode integration ensures that patient samples are tracked continuously, satisfying CLIA and ISO 15189 chain-of-custody requirements automatically.
- Transcription is Eliminated: Seamless integration with instruments across all disciplines — from molecular to microbiology — removes the risk of human data entry errors.
- Compliance is Built-In: A genuine clinical LIMS features an architecture anchored by immutable audit trails and secure digital signatures to meet CLIA, HIPAA, 21 CFR Part 11, and CAP standards.
- Automation Drives Consistency: Configurable custom workflows automate repetitive tasks like sample receipt and report generation, enforcing standardization across diverse testing processes.
- Turnaround Time is a Clinical Metric: Detailed analytics and real-time customizable reporting ensure that critical diagnostic data reaches healthcare providers faster, improving patient care.
- Security Enables Collaboration: Robust security protocols (encryption, RBAC, MFA, SOC 2, ISO 27001) allow for secure, cloud-based remote monitoring and multi-site professional collaboration.
Final Thoughts
The mandate of a diagnostic laboratory is to provide accurate, timely, and actionable medical intelligence to healthcare providers. Yet, decades of clinical laboratory quality literature consistently prove that the most profound threat to this mandate is not analytical imprecision, but rather preanalytical identification failures and manual data management errors.
When a diagnostic laboratory continues to rely on manual sample tracking, handwritten logs, and human transcription of instrument data, it is actively ignoring the dominant, repeatedly studied category of clinical laboratory error.
A diagnostic laboratory's data management infrastructure is therefore not a secondary administrative concern. It is the primary control point for patient safety. A purpose-built clinical diagnostics LIMS secures the chain of custody, automates data capture, and enforces regulatory compliance through system architecture, removing the burden of manual vigilance from clinical staff.
By eliminating the manual processes that introduce risk, laboratory professionals are freed to focus entirely on diagnostic analysis and clinical decision-making. We invite laboratory directors, CLIA compliance officers, and hospital administrators to critically evaluate their current data infrastructure against this framework, ensuring their systems are truly equipped to protect both sample integrity and patient outcomes.
Continue Reading
- How to Prepare Your LIMS for an FDA Audit: A Practical Checklist
- Achieving ISO/IEC 17025 Compliance: How a Modern LIMS Simplifies Accreditation
- Signs Your Legacy LIMS Is Costing You More Than You Think
- A Complete Guide to LIMS for ISO 17025 Accredited Testing and Calibration Labs
- From Reactive Testing to Predictive Intelligence: AI-Powered LIMS for Food and Beverage Laboratories



 (1) (1).webp)


.webp)